Blood Flow Restriction – Wat is dit?
In Groningen zijn wij de eerste en enige fysiotherapie praktijk die gelicenseerd is om te trainen met Blood Flow Restriction.
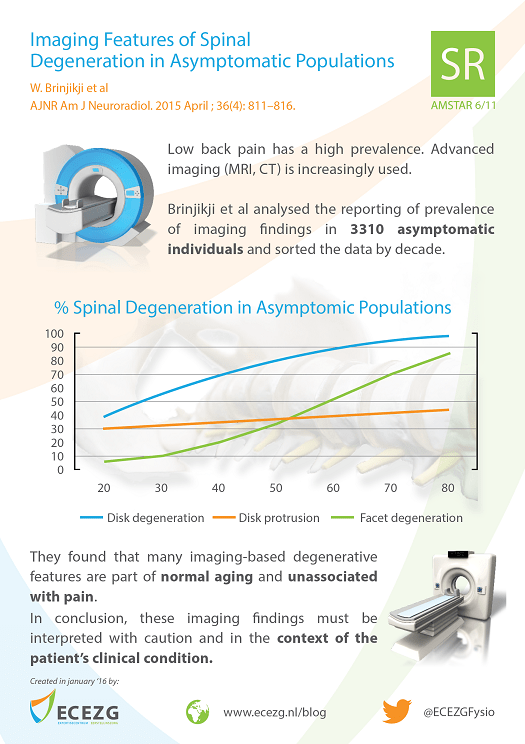
Blood flow restriction training (BFR) is een “nieuwe” manier van training die zijn opmars begint te maken binnen de fitness en paramedische wereld. Een grote hoeveelheid wetenschappelijke artikelen laat zien dat BFR hypertrofie en kracht toename kan genereren bij zeer lage belasting (20-30% van individuele 1RM) tegenover conventionele training met belasting van 75% of hoger van 1RM.
Waar wij als therapeuten nu nog gebonden zijn aan de reguliere fysiologische wetten van weefsel herstel, toont BFR zich als een ware game changer in de revalidatie wereld.
Blood flow restriction zorgt er voor dat er een toename is in de muscle proteïne synthese. En dat al bij zeer lage belasting op het lichaam.
Maar wat is Blood flow restriction nu precies? En wat doet het?
BFR is trainen onder arteriële occlusie (50% bij biceps, 80% quadriceps) en 100% veneuze occlusie. Kortweg, je verminderd de doorbloeding gedeeltelijk. Je maakt gebruik van een speciaal apparaat, een persoonlijk tourniquet systeem. Deze meet continu de bloeddruk en gebruikt dit om de mate van occlusie aan te passen. Dit zorgt uiteindelijk voor de cellulaire zwelling in de spieren (Loenneke et al., 2012; Abe et al., 2008; Wilson et al., 2012). Deze zwelling is onderdeel van de verhoogde proteïne synthese. Dit is dezelfde “pomp” die je ook voelt na conventionele krachttraining.
Voordeel bij BFR is dat we nog maar 20-30% van dezelfde 1RM nodig om deze cellulaire prikkel te geven, zonder daarbij zoveel microtrauma (spierschade) te maken zoals bij conventionele hypertrofie training. Dus minder spierpijn en kortere herstel periodes. Daarnaast kan het toegevoegd worden aan het einde van conventionele training, om ‘extra’ te trainen.

Toepassing
Zowel binnen de reguliere trainingen van een sporter als bij de revalidatie na blessures of operatie kan BFR worden ingezet. Zo kan de sporter al 1 dag of 1 week na blessure of operatie weer krachttraining doen. Deze training kan met minimale belasting en zo het gat overbruggen naar conventionele krachttraining. (Takarada, 2000)
BFR is een ontzettend goed middel om atrofie na operatie tegen te gaan. We zien in de literatuur terug dat de proefpersonen binnen 6 weken weer spiermassa opbouwen binnen 10% verschil met, of gelijk aan de niet geopereerde zijde.
Dat zijn gigantische sprongen voor de eerste fase van revalidatie. Nu kan na 6 weken al gestart worden met normale krachttraining omdat kracht, spiermassa en collageen sterk genoeg is voor die belasting.
Veiligheid
Om de veiligheid te waarborgen binnen de revalidatie setting zijn er een aantal contraindicaties opgesteld rondom Blood flow restriction training. Zonder uitgebreid intake en onderzoek kan het gebruik van BFR risico’s met zich mee brengen.
In de volgend blogs zullen we dieper in gaan op de fysiologie achter BFR. De veiligheid van BFR zullen we bespreken en hoe de toepassing is binnen je revalidatie traject of eigen krachttrainingen.